



The "angels" of Chernobyl
Yves Lenoir1, Enfants de Tchernobyl Belarus
February-March 2022
"Rieux - It is hardly believable, but it seems to be the plague"
Albert Camus,The Plague
"People are always slow to believe in the plague.
Because people deny them, plagues spread".
Orhan Pamuk, author of The Nights of the Plague
Introductory summary
International reports on the health consequences of the Chernobyl accident deny most of the causal relationships that objective examination of the statistics requires. Finally, apart from 50 fatal cases of acute radiation syndrome and a few thousand cases of thyroid cancer in the infant population of Belarus and Ukraine, there is no justification for attributing the spectacular deterioration in the health of the populations living or having spent long periods of time in the most contaminated regions to the radioactive fallout of the accident.
The most denied consequences of the accident, not even mentioned, except in compilations that are not recognised because they do not conform to the official conclusions, concern everything related to the birth rate. No statistics in this area are included in the "authoritative" reports of the UNSCEAR, the ICRP, the WHO and in their repetition by the IAEA, the OECD and other organisations closely or remotely linked to the atomic industry and to the exposure of the population to radiation, i.e. to "radiological protection". Detailed statistics for each country on birth rates, infant mortality rates, foetal deaths and therapeutic abortions are available on the internet, digitised, and can be easily copied and pasted into spreadsheets.
We collected data from about twenty countries, whether or not they were affected by the fallout from Chernobyl and/or whether or not they had sent liquidators to the accident site and the areas to be decontaminated. After sorting out the anomalies in the historical curves of the indicators, weighted by the population and birth rate figures, and then assessing the order of magnitude of the cause-and-effect relationships in the various cases presented by the data from these twenty countries, we selected seventeen of them, two of which were "control" countries, since they had obviously not suffered any detectable consequences in the field of human reproduction.
By "angels" we mean fetuses destroyed in therapeutic abortions (duly recorded) and spontaneous fetal deaths. By "near-angels" we mean all the little people who died before reaching the age of one, those who fall into the category of "infant mortality". Of course, the count only covers the anomalies revealed by the shape of the curves.
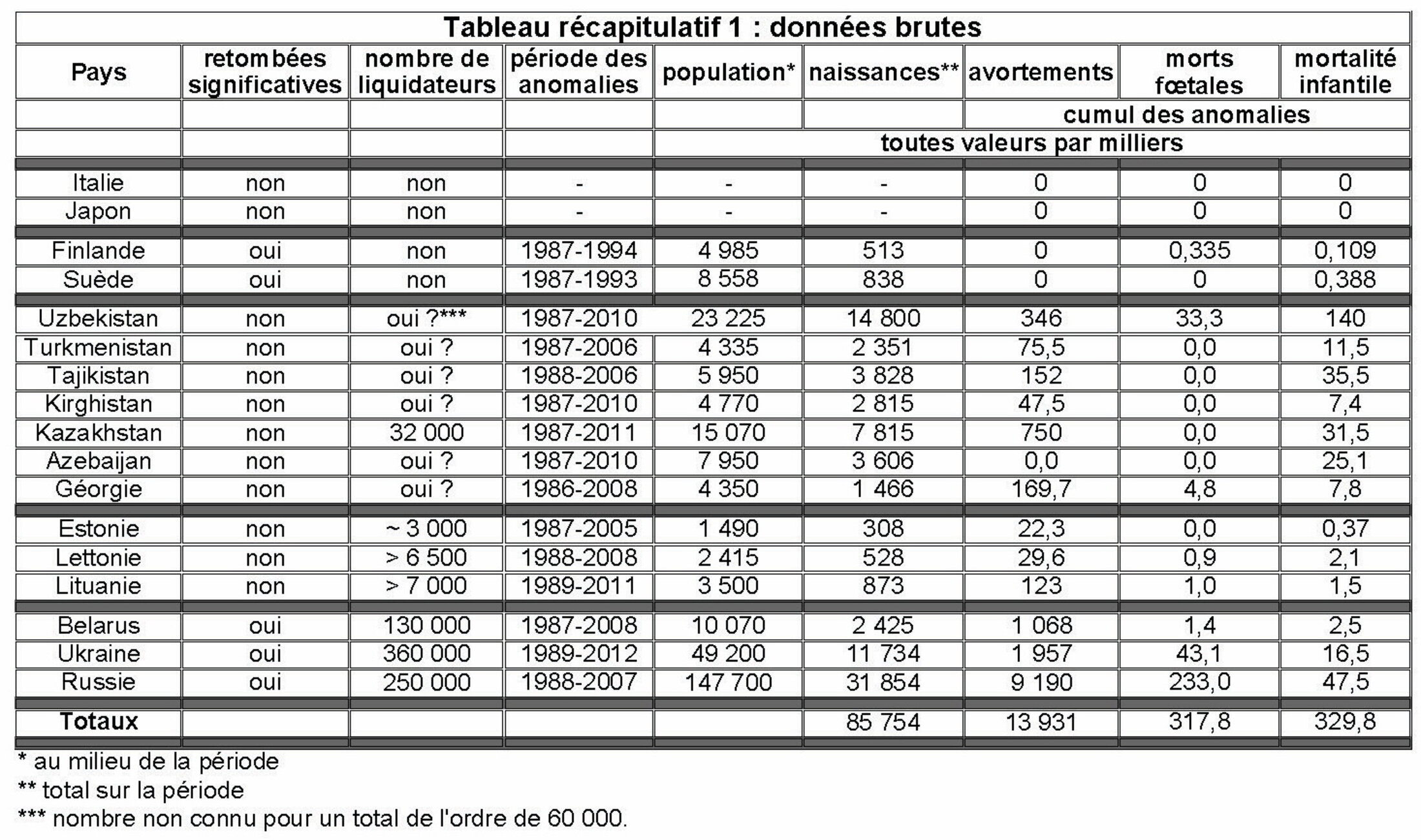
A list of the 17 countries and a summary of the raw results for them can be found infra. The totals of these results are in three figures:
- number of "near angels": 329,000 ;
- number of "spontaneous angels" per fetal death: 317,000;
- number of 'angels' produced by therapeutic abortion: 13,931,000.
It should be borne in mind, as the curves show, that the duration of the anomalies can be as long as twenty years and that, in total, the selected countries have a population of 293.5 million and have recorded 85.7 million viable births during the historical phase of the anomalies, which differs from country to country according to its relationship with Chernobyl.
This small study measures the extent of the ignored consequences of a major radiological crisis produced by a near-maximum atomic disaster, the equivalent of a tactical atomic war in which a few hundred so-called "theatre" weapons would explode at very low altitude, or even on the ground.
Evidence collected on site from Dr Raisa Misura in Stolin and two nearby villages.
From the UN Bulletin, Belarus office, January-February 2008 (p. 4):
"Currently, Stolin district has one of the highest birth rates among rural areas of Belarus. 1120 children were born there in 2007, or 13.3 per thousand inhabitants.
However, according to the deputy director of the Stolin Central Hospital, Raisa Misura, 60% of women of childbearing age (18-40) and over 84% of pregnant women have one or more diseases. Therefore, the birth of a perfectly healthy child is a rare event. Almost 90% of newborns are in health groups II or Ill2.
"The low level of knowledge and lack of practical skills in radioecology require additional efforts," said Ms Misura."
On 8 July 2016, Dr Raisa Misura3 received us for a good hour in her office at the Central Hospital of the Stolin raion4, a town located 250 km west of the Chernobyl NPP. At the time, she was5 the deputy chief physician for the medical care of the rural population and the organisational and methodological work. After graduating from the University of Pediatric Medicine in Leningrad in 1984, then a maternity leave and two years of internship at the Reshitsa dispensary, a few kilometers south-west of Stolin, she was assigned to the Stolin hospital on 1 August 1986. She has thus followed the evolution of the health of the population of the raion without interruption since the radioactive fallout of the accident at the beginning of May 1986. She has contributed to the establishment of detailed and precise medical statistics, year after year, between 1986 and 2018, which she sent to us in two parts, a few weeks after our interview, then a supplement at the beginning of 2019.
Knowing that the state of health of the population, and in particular of children, had been deteriorating steadily for several months after the accident, we had prepared a set of questions concerning her observations and the means implemented to limitthe radioactive damage to health.
She told us that the local medical profession only gradually became aware that the accident was not without consequences for people's health. An extract from our exchange:
"Before 1989, before the publication of the first map of radioactive contamination in the newspaper "Pravda", nobody knew anything in particular. And how did things work in your country?
- You know. It's difficult to remember now. But... I don't remember that any special medical measures were taken... Being a district paediatrician, I worked intuitively. You see that the number of leucocytes has decreased a lot in the blood, there is the appropriate therapy. Some medical measures were taken, maybe also for the decrease of the dose loads. Maybe they were taken here in the hospital. But we didn't know."
To a question about the risk of radiation-induced malformations, of which everyone in these contaminated regions had been aware of painful cases since the autumn of 1988, either directly or through the revelations of the investigative journalist Vladimir Kolinko in the newspaper Sovietskaya Belorossiya, she admitted as if with regret:
"Let's start with the fact that young mothers' schools existed before the Chernobyl disaster in Soviet public health. Why did they exist? Because, as they say, he who is warned is protected. All this means, for our planning, that in the school for young mothers another component has appeared, namely radiological protection. So that the radioactive dose to the pregnant woman is reduced as much as possible.
Ultrasound screening has certainly helped to solve the problem of fewer children being born with congenital malformations. Because some of them were medically interrupted during gestation."
So there were clearly unwanted terminations of pregnancy following the revelation of malformations visible on ultrasound. How many? And what about the undetectable malformations? How was this part of the aftermath of the disaster dealt with in the official reports? What about fetal and infant mortality? These are huge questions that have not been the subject of any truly scientific work, as we shall discuss.
These matters are sensitive; dealing with them touches each and every one of us in our intimacy and awakens grief. Time has passed, gradually erasing the pain and drowning the bad memories in a soothing fog. Respect and discretion are required.
This is why we decided to look at the statistics, knowing that we have a solid core, those of the Central Hospital of Stolin: 32 years, the film of the evolution of pathologies and demography in a population of a hundred thousand souls. From there, we will broaden the perspective to the ex-USSR republics because, even if not directly affected by the fallout of the radioactive plumes from Chernobyl, they all sent battalions of "liquidators" to the site of the power plant and to the highly contaminated un-evacuated land. The indicators examined will be compared with their equivalents in different countries, some of which have suffered significant fallout (Sweden, Finland, etc.) and others which have not been significantly exposed.
At the end of this work, we will have an indicative figure - neither by excessive cherry picking nor by default in order to exonerate radioactivity from obvious statistical anomalies - of the number of angels6 that Chernobyl sent to populate the celestial limbo. It will remain indicative because the scale of the multi-disciplinary scientific retrospective study required to consolidate it will dissuade any funding. It is reasonable to bet on this.
A campaign of therapeutic interruption of pregnancies with visible malformations should not be surprising when a major radiological crisis is underway. However, as not all malformations are detectable, malformed children will be born, and this will be a family tragedy that must be dealt with.
The day before and the morning of our interview with Raisa Misura, we met biology teacher Liliya Bovkunovich from the Diatlovichi school and nurse Praskovya Polukoshko, who is responsible for care in the village of Olmany. Both villages are part of the Stolin raion. Both spontaneously mentioned cases of spastic diplegia among the child health problems that concerned them, 7 in Diatlovichi in a population of 350 children and 4 in Olmany in a population of 98 children. An accident during childbirth leading to irreversible brain damage is one of the causes of spastic diplegia, a motor paralysis of the four limbs. In addition, there are prenatal causes, in utero, which are listed in the scientific literature, including irradiation; one medical document even mentions "Chernobyl type". Our two interlocutors are well-informed professionals and added that the situation "was not normal". Especially since the Belarusian health system has always been of a high standard, equivalent to that of the Baltic States and Finland according to international indicators. It is difficult to dismiss the Chernobyl cause, as all official UN and international reports (WHO, UNSCEAR, OECD, etc.) on the health consequences of Chernobyl do.
Indeed, the contamination checks on forest and vegetable products - essential food resources in the rural regions of Belarus, but also in Ukraine and Russia - reveal levels that are often "stratospheric", up to 350 kBq/kg for dried mushrooms (legal marketing limit: 2.5 kBq/kg) and 56 kBq/kg for fresh mushrooms (legal limit: 370 Bq/kg), and figures to match for berries and game However, as Liliya Bovkunovich, who is also in charge of the only radiological food control equipment in the village of Diatlovichi, told us, barely 30% of the products of forest and vegetable harvests are subject to measurement. That pregnant women irradiate their unborn children by eating radioactive food is not a hypothesis but a statistical reality. Raisa Misura's statement in the UN newsletter in Belarus is illustrated by the fact that in the raion where she is one of the medical officers, the reported levels of spastic diplegia alone are more than 20 times higher than before the accident or elsewhere in the world.
Some historical and contextual elements
Chernobyl imposed major population movements, all of which were delayed. For example, the evacuation of the town of Pripyat, located 2 km north of the power plant with a southerly wind at the time of the accident, did not take place until more than 36 hours after the explosion, when the external radiation level in the town was approaching the 1 Sv limit for the involvement of troops in an atomic conflict. The notes of the KGB cell in Chernobyl mention 137 cases of acute radiation syndrome, of which about 50 were children, in the city's population. Acute radiation syndrome occurs after a dose of more than 2 Sv (the short-term lethal dose is 6 Sv). Testimonies collected by the American Glen Alan Cheney in the early 1990s among Pripyat evacuees relocated to Kiev suggest that there were other cases of acute radiation syndrome, but even more of chronic radiation sickness, among the inhabitants who left by their own means, i.e. in their private cars, as the number of buses sent to evacuate the city was insufficient. The evacuations of the villages in what was to become the 'exclusion zone' took place after 1 May, when most of the radioactive fallout, largely triggered by the airborne assets of the Soviet military air force, had already occurred.
About 160,000 people were evacuated during this first wave. To their external irradiation must be added the internal irradiation caused by the inhalation of radioactive gases and particles and the ingestion of contaminated food. There are enough testimonies about the total absence of preventive measures (in order not to cause panic) to affirm that in the spring of 1986, all that nature and family gardens were beginning to offer was consumed.
At the same time, tens, then hundreds of thousands of 'liquidators' from all over the Union7 flocked to the site of the power plant and to the areas to be decontaminated. A certain proportion of them were women. All of them then returned to their homes. Those who were not ill, or not yet ill, sought to have children, and did.
Three years later, in March 1989, pushed to the limit by press reports showing that the health damage to livestock was increasing and beginning to be felt by the population, especially children, the Soviet authorities published maps of the fallout throughout the Union and then decided to organise a new round of evacuations involving 250,000 people from highly contaminated areas.
As a result, more than a million people who had been particularly exposed to the radioactive fallout from the accident and/or who had participated in the so-called "liquidation" of its consequences were dispersed and relocated, sometimes far from their home area.
Since the early 1950s, the Belarusian Ministry of Health has had a department responsible for recording all malformations. The data collected and published shed light on the influence of population movements on the dynamics of the phenomenon. Below is a summary of all the data:
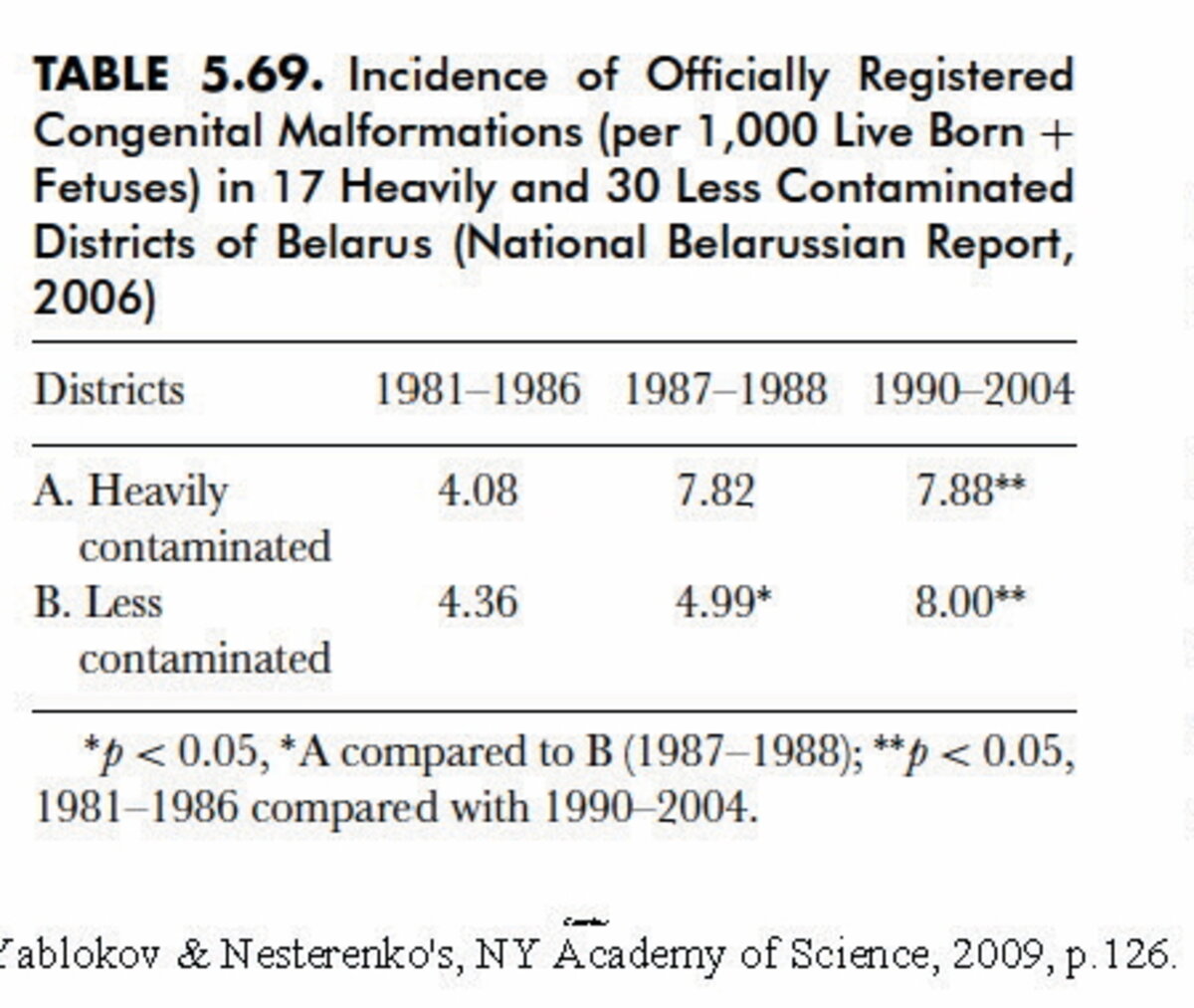
Comment 1:
- before the major evacuation of 1989, the rate of malformations increased particularly in the most contaminated regions, and relatively little in the least affected regions;
- after this second wave of evacuations, the mixing of populations resulted in an influx of at-risk couples into the less affected regions, where they found refuge. Carrying the mark of Chernobyl in their bodies, they contributed to averaging the trend of the national curve of the rate of congenital malformations... The majority of older people remained.
- which was exploited by international bodies and 'experts' from official 'radiological protection' organisations to assert that this doubling of congenital malformations being more or less the same throughout the country, it should not be linked to the Chernobyl accident! Or how to scientifically protect the aura of atomic energy after a major radiological disaster.
Some reports provide partial data to keep in mind when reading the rest of this paper:
- the Storch report states that a Ukrainian cohort of 253,000 "liquidators" and 165,000 evacuees produced 643,000 children;
- a study of a cohort of 'liquidators' found a rate of birth defects in their offspring six times higher than the population average;
- partial statistics reveal that the average age at death of the 'liquidators' employed on the site, particularly in the construction of the sarcophagus, is less than 50 years;
- only epidemiological studies based on a precise distribution of "typical radiological pathways" would have made it possible to identify the teratogenic effect of the doses inflicted by Chernobyl. Ignorance has been legally and methodically preserved.
Indeed, the "authorised" assessments of the effects of Chernobyl fallout do not include, without giving reasons, the cocktail8 of short- and medium-period radionuclides to which all these liquidators and inhabitants of the evacuated zones were exposed and which they ingested, day after day, without having the slightest idea of it. The pathologies developed by the most exposed liquidators and inhabitants of Pripyat clearly show a massive multiform contamination by several radio-nuclides. As dosimetry is deficient, none of the victims (except for thyroid diseases, which are so specific that they cannot be unrelated to I131) has been officially recognised as injured by radiation.
The case of Belarus
Belarus is the country that suffered the greatest radioactive fallout and had to evacuate the largest number of villages. Let us take it as a starting point for the analysis of the effects of Chernobyl on demography. Let us start from the curves of the raw data of the abortion rate according to several sources. It should be mentioned here that abortion has been an important means of birth control in all communist countries. As a result, being subject to no legal restrictions, all procedures were performed in the medical environment and were therefore duly registered (but not necessarily published, as we shall see). Also, after the break-up of the communist bloc, the legislation sometimes changed completely, so that there was a sudden change in this rate. Poland offers an emblematic example, with the rate of (registered) therapeutic abortions rising from 20/100 births in 1981 to almost zero in 1993 (one can imagine where things are going then). An opposite pattern is observed in France: a rapid increase in registered abortions after the enactment of the Veil law...
This means that the matter is complex and multifactorial. The interpretation of anomalies must therefore be carried out with circumspection and in the light of as many components of the context and the changes that have occurred as possible.
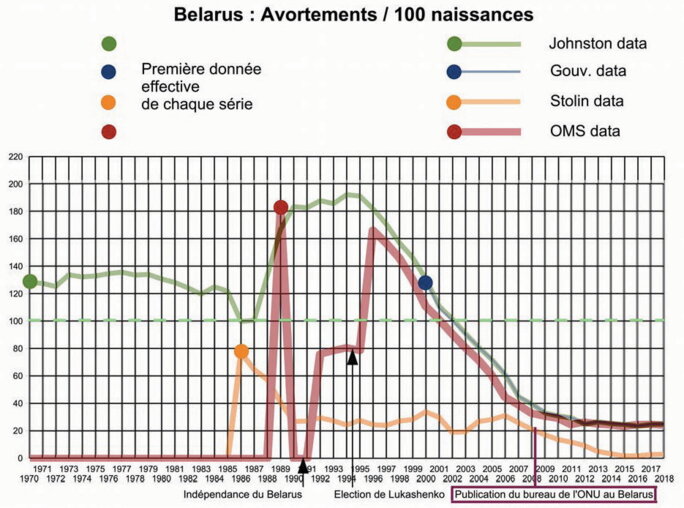
A. Therapeutic abortions
Agrandissement : Illustration 2
These curves, and their differences, speak volumes.
1. the curve from the W. Robert Johnston9 archives is uninterrupted since 1970. Its reliability is guaranteed by the conformity of the values published by the Belarusian Ministry of Health (from 2000 onwards) and by those communicated to the WHO in 1989, then from 1996 onwards by the government of A. Lukshenko). The statistics from the central hospital in Stolin clearly call for a detailed analysis, which we will do below;
2. the political upheavals of 1990 and the election of Alexandr Lukashenko as President of the country clearly affected the transmission of data to the WHO. It is notable that the first post-independence government was reluctant (out of modesty?) to provide the international organisation with the actual figures. However, Robert Johnston managed to obtain the full data;
3. between 1985 and 1987 the rate of therapeutic abortions decreased slightly. The Chernobyl effect had clearly not yet been fully appreciated by doctors (as evidenced by the numerous photos of children with monstrous deformities taken in 1986 and 1987 and reproduced in newspapers and media of the time, both in the USSR and outside the Union);
4. as Raisa Misura points out, the systematisation of ultrasound examinations subsequently made it possible to eliminate fetuses with visible malformations;
5. Can we consider that all the abortions above the rate of 100/100 births (1987 value) carried out between 1988 and 2002 were motivated by malformations detected by ultrasound? Many may have been motivated by fear. In any case, during this 15-year period, the number of Belarusian "angels" sent to heavenly limbo because of Chernobyl amounts to 1,068,373;
6. Belarusian demographics declined after 1990, with the country losing about 800,000 people in the following 15-20 years, and the trend remains downward to the present day, while the abortion rate has fallen sharply, indicating that the means of birth control have become more diverse.
We will return to the gross figure concluding point 5. after comparing the share probably attributable to the offspring of the liquidators in the other Union republics with that which should be sought in their populations, their culture, their religion and the situation in which they lived.
It is now necessary to evaluate the less severe disturbances that Chernobyl may have caused in the historical series of fetal and infant deaths (from conception to one year after birth).
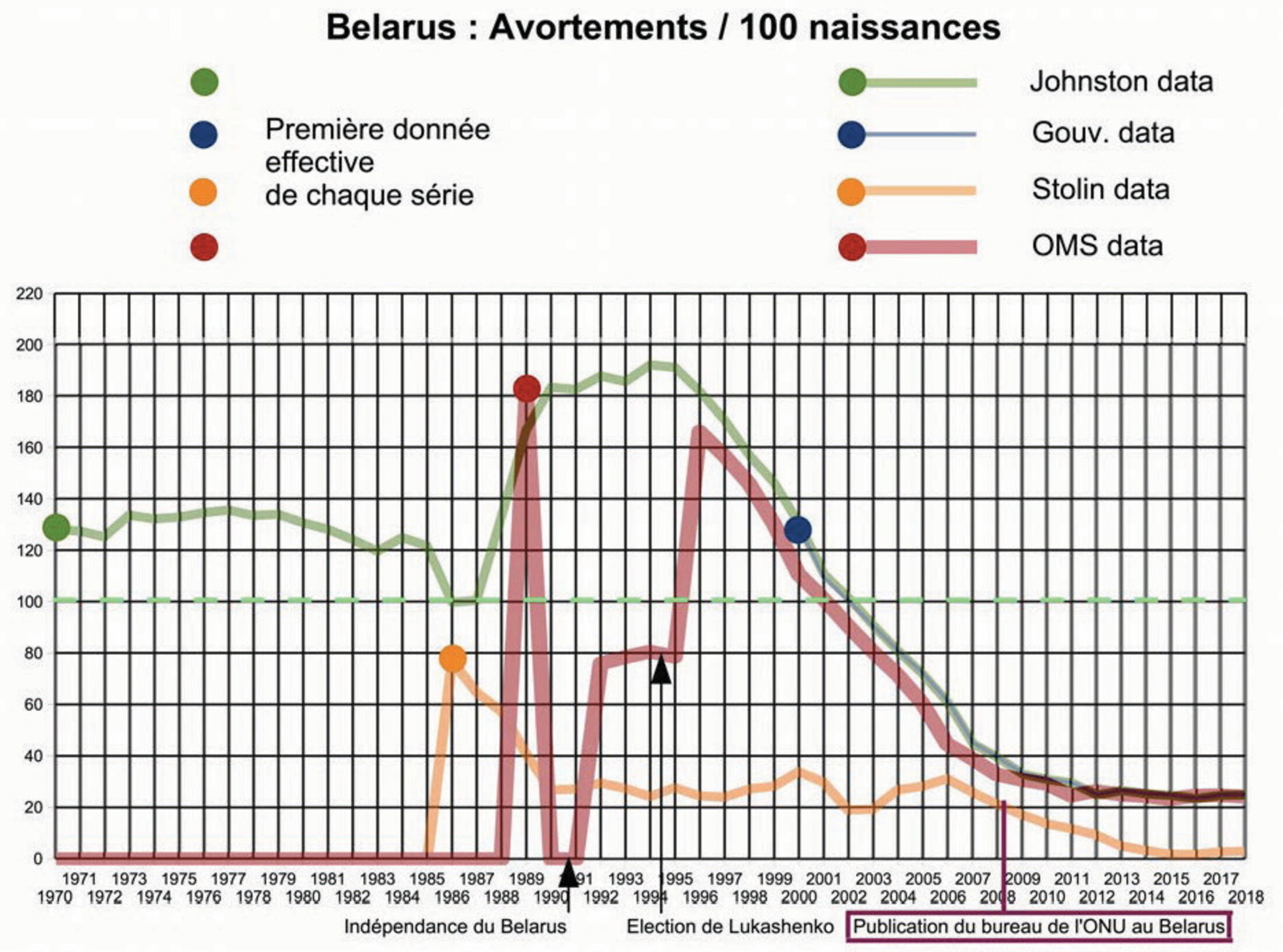
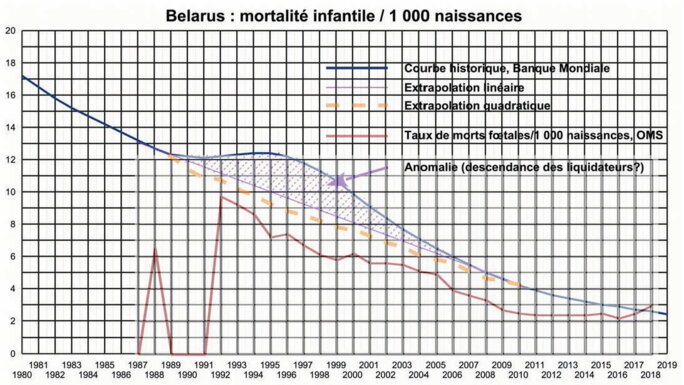
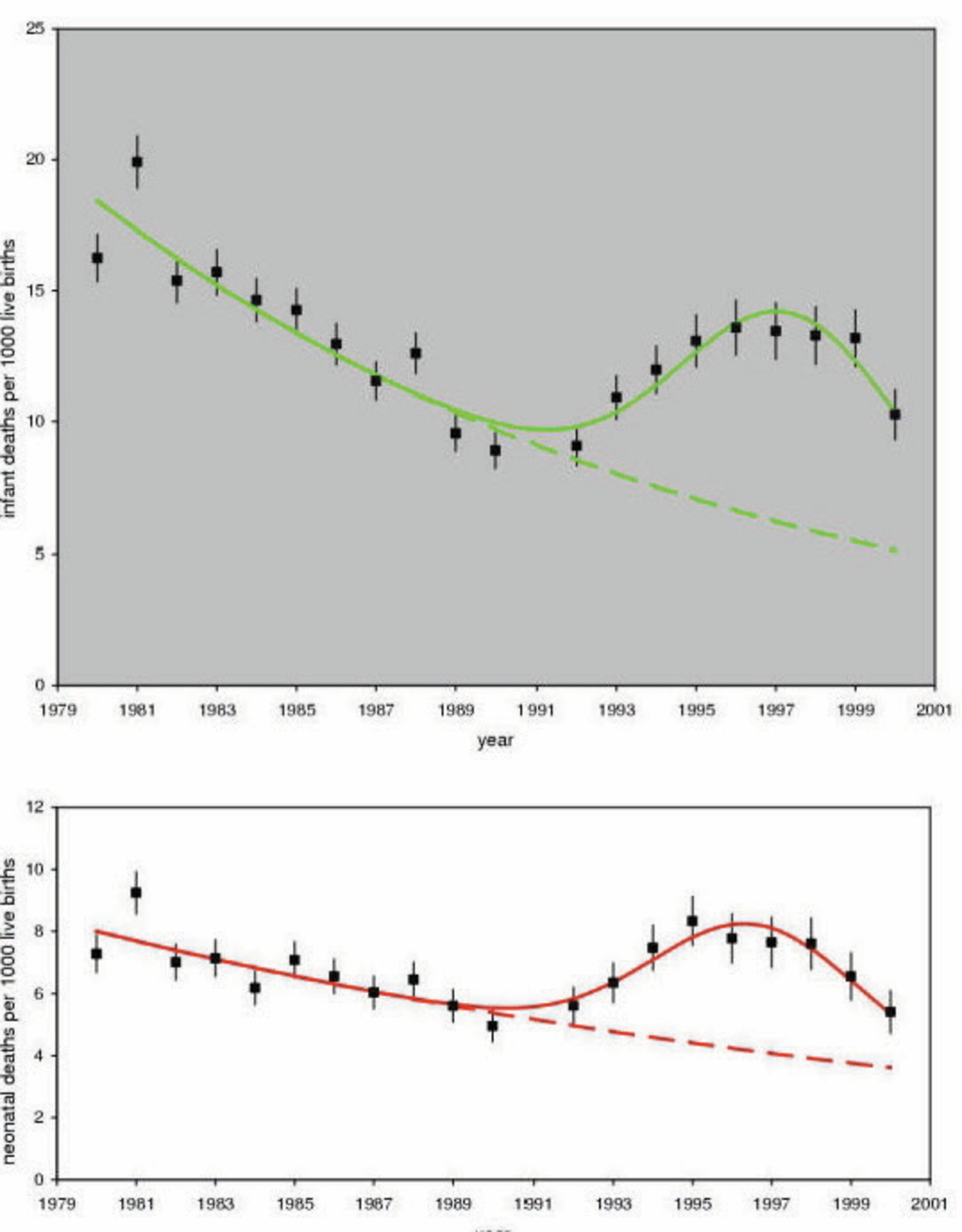
B. Fetal and infant mortality
The WHO fetal death rate curve lacks the years most needed to analyse the role of Chernobyl, those prior to 1988 and the three years 1989-1991. However, if the 1988 data is reliable, as can be deduced from the abortion rate graph where the value provided to WHO in that year coincides with that in the Johnston archive, then roughly the same assessment procedure can be applied as for the excess of therapeutic abortions. We are forced to a default assessment because of the three missing values: any rate above 6/1000 births is considered an excess.
As for the infant mortality rate curve (between 0 and 1 year), it shows an anomaly characteristic of all the republics that sent liquidators to Chernobyl (even if these republics did not suffer radioactive fallout). The liquidator cause at Chernobyl is reinforced by the absence of anomaly in the countries outside the former USSR that suffered fallout (see below for all the demonstrative graphs).
Agrandissement : Illustration 3
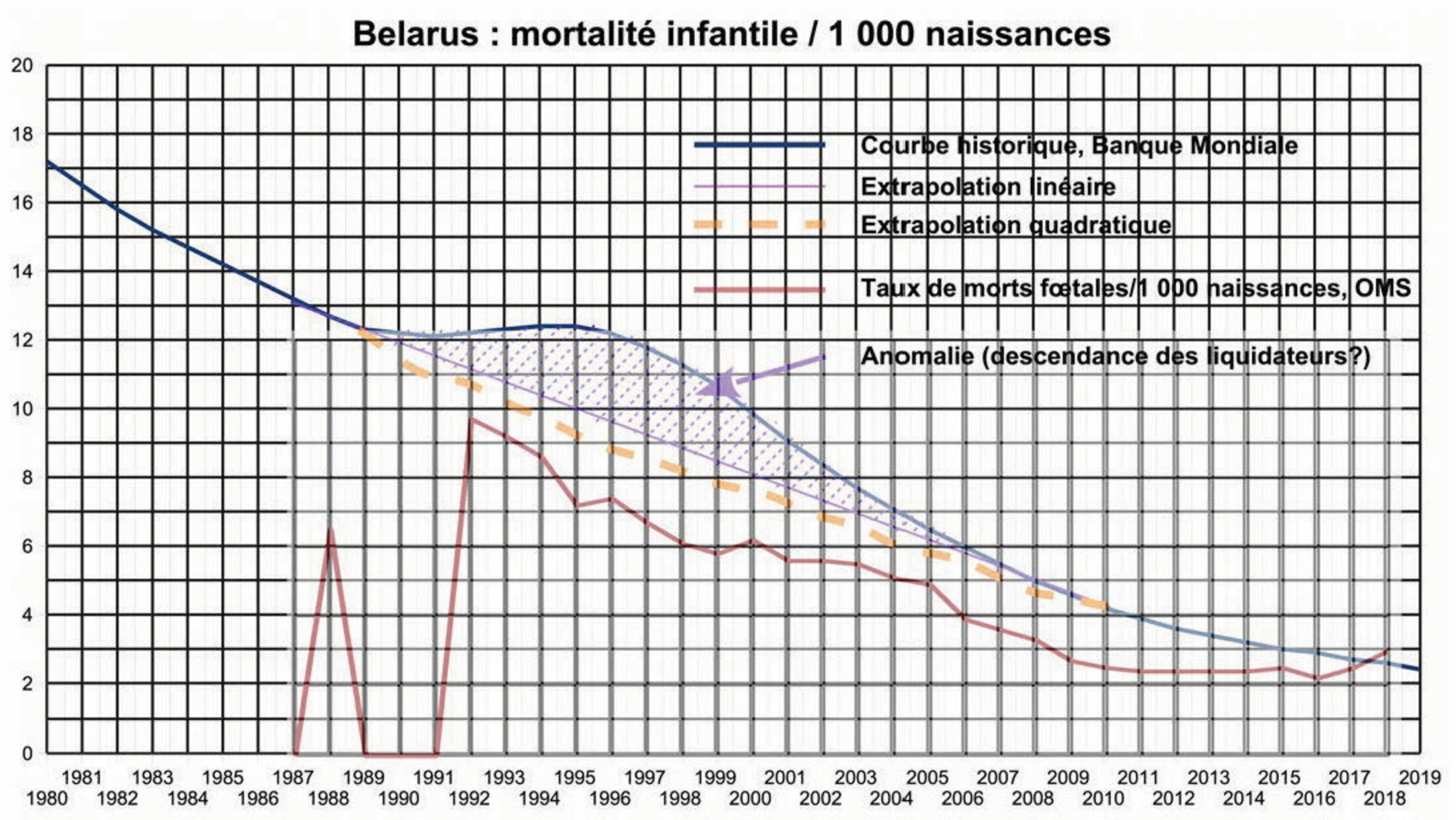
In relation to the number of births, the excesses of the two types of death are
- between 2,200 and 2,900 for infant mortality, depending on whether the linear or quadratic approximation is adopted
- around 1,400 for fetal mortality.
It can be seen that, in relation to the abortions necessitated by Chernobyl, the excess fetal and infant mortality is marginal: a default total of about 4,000 deaths (0.4% of a total of around one million). The fact that the descendants of the liquidators are affected, adding bereavement to the many pathologies, disabilities and premature deaths (before the age of 50) affecting this population, is particularly dramatic.
C. Is the Stolin case an exception?
The comparison of the statistics of the Stolin Hospital with the overall Belarusian statistics inspired Alexey Nesterenko, the Director of the independent BELRAD Institute, with which the international association I chair, Children of Chernobyl Belarus, has had close relations for over twenty years, to make the following comment:
"One of the reasons for the high birth rate in the Stolin radius, I suppose, is because there is the richest private agricultural sector in Belarus. You see greenhouses for cucumbers and strawberries. That's why young people don't go to the big cities as usual, but stay in the villages and are involved in business. Secondly, the richer villages with many young people have a majority of Baptists. Alcohol and birth control are forbidden there."
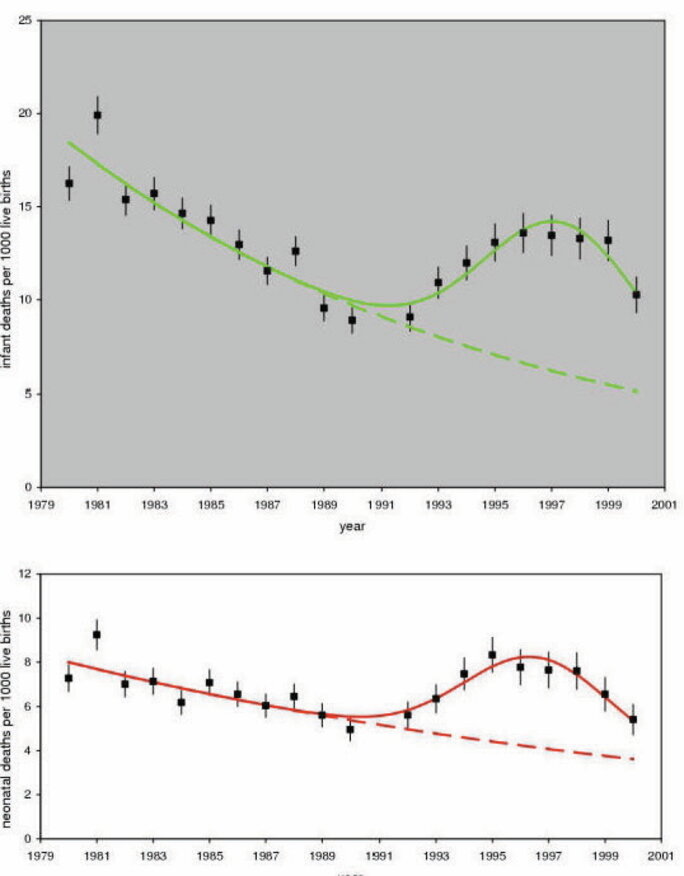
Here he points to crops that do not concentrate Cs137, as do berries and forest mushrooms. However, the rate of malformations remains very high, more than 35 years after the accident, and the health status of the population, adults and children, remains as bad as in the rest of the country. Regarding birth control, the official data per oblast do not show any decisive indication to support his remarks:
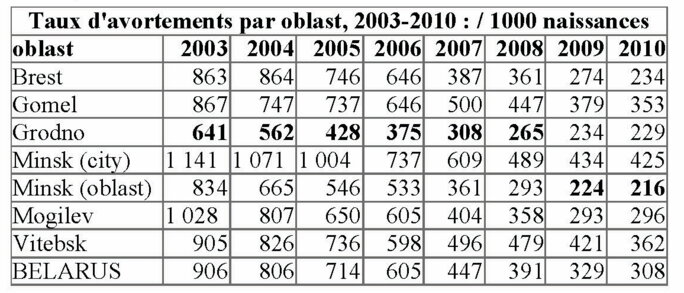
Agrandissement : Illustration 4
Minimum values are shown in bold. These are data from the Johnston archive, which is the only one per oblast that has apparently been digitized and published on the Internet. The rate of therapeutic abortions in Brest Oblast, which includes the Stolin Raion, is below average and therefore does not stand out for its low level of birth control through therapeutic abortions.
The exceptional birth rate results in Stolin raion, as recorded since 1986, are rather a testimony to the fact that the population of Stolin rayon is 80% agricultural and, indeed, predominantly Baptist - two reasons for the relative lack of birth control, and to the remarkable work of Dr Raisa Misura in the services she has directed. This is probably why she was singled out in the January-February 2008 newsletter of the UN office in Belarus. The case of this department is an exception.
The general decline in this practice accelerates after 2006 towards the end of the Chernobyl liquidation period, but also due to the evolution of birth control techniques. By the end of the decade, abortion rates are gradually reaching the values observed in most developed countries, except those where abortion is prohibited and therefore no credible statistics are published.
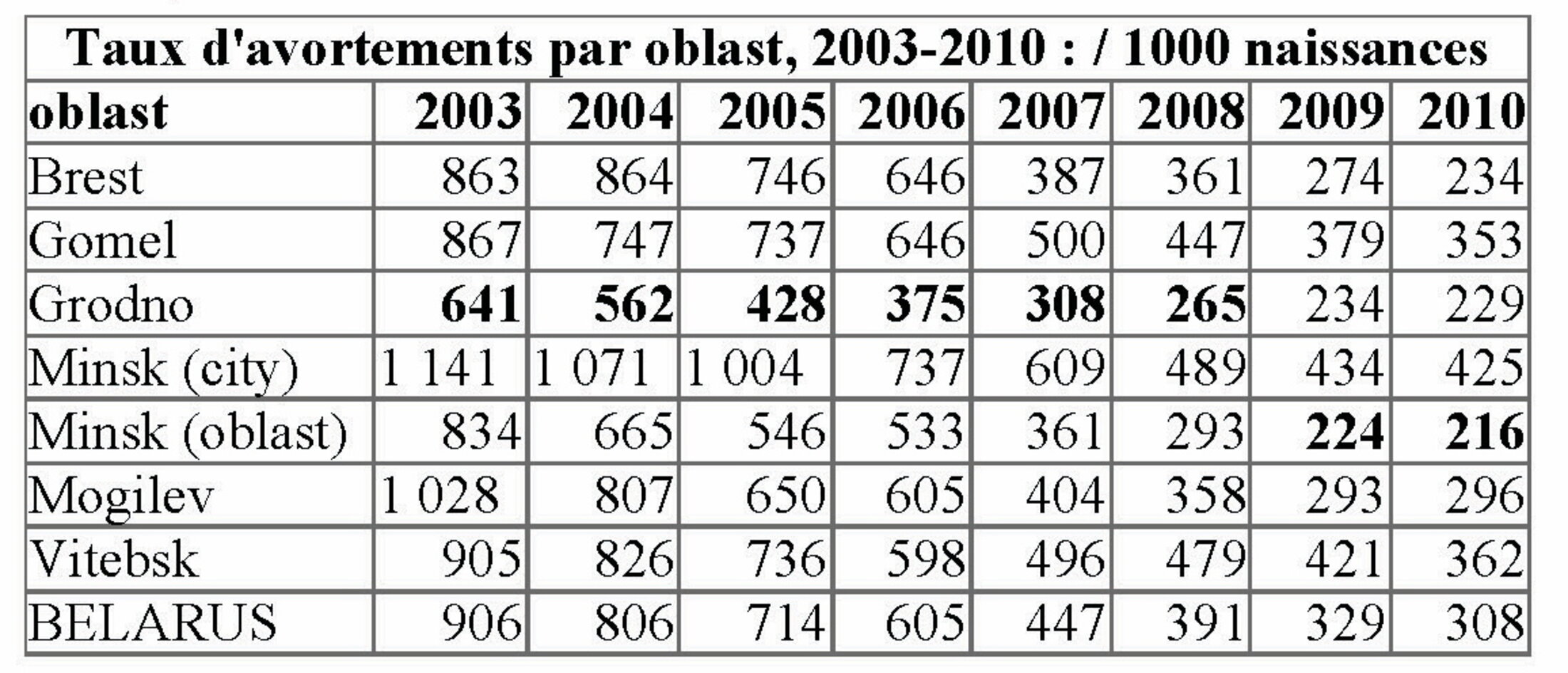
Finally, two official graphs showing the neo-mortality and infant mortality indicators in the Mogilev oblast, one of the most affected by the fallout, with the exception of the city of Mogilev itself, preserved by aerial management of the radioactive plumes).
Agrandissement : Illustration 5
These two curves, compared with their counterparts for the whole of Belarus (see above), show that the origin of the abnormalities is not necessarily entirely in the descendants of the liquidators and evacuees, but may be partly the consequence of environmental contamination. That said, the analysis can hardly go any further because only a detailed study would make it possible to clarify matters, a study that would take into account the proportion of the region's inhabitants who participated in the liquidation of the accident, the evacuees who were relocated to this oblast, and the contamination of the environment
The bottom line: national averages tend to blur the radioactive cause of the anomalies. The detailed global study aimed at revealing the health after-effects of Chernobyl remains to be done.
The more time passes, the more expensive and less feasible such a study would be. The denial of the effects of Chernobyl is thus essentially fed by the strategy of the UN organisations, UNSCEAR, WHO and IAEA. The consequence is that the passage of time is allowed to cut clear links between cause and effect. The freedom to deny the reality of these links is scientifically justified. However, careful country-by-country comparisons help to identify the causes.
The other republics of the former USSR
Let us start with the infant mortality curves in the other republics, all of which sent liquidators to Chernobyl, although for some the number is not known. We know that there were some, notably from the lists on the Chernobyl memorials in the central barracks, alongside those of the dead in the Great Patriotic War and in the Afghan War. Fetal mortality curves are presented as in the Belarus example.
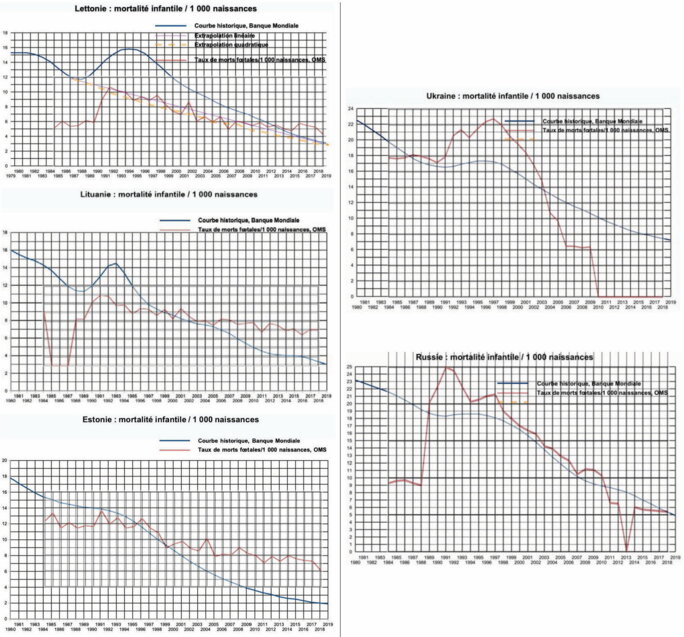
Agrandissement : Illustration 6
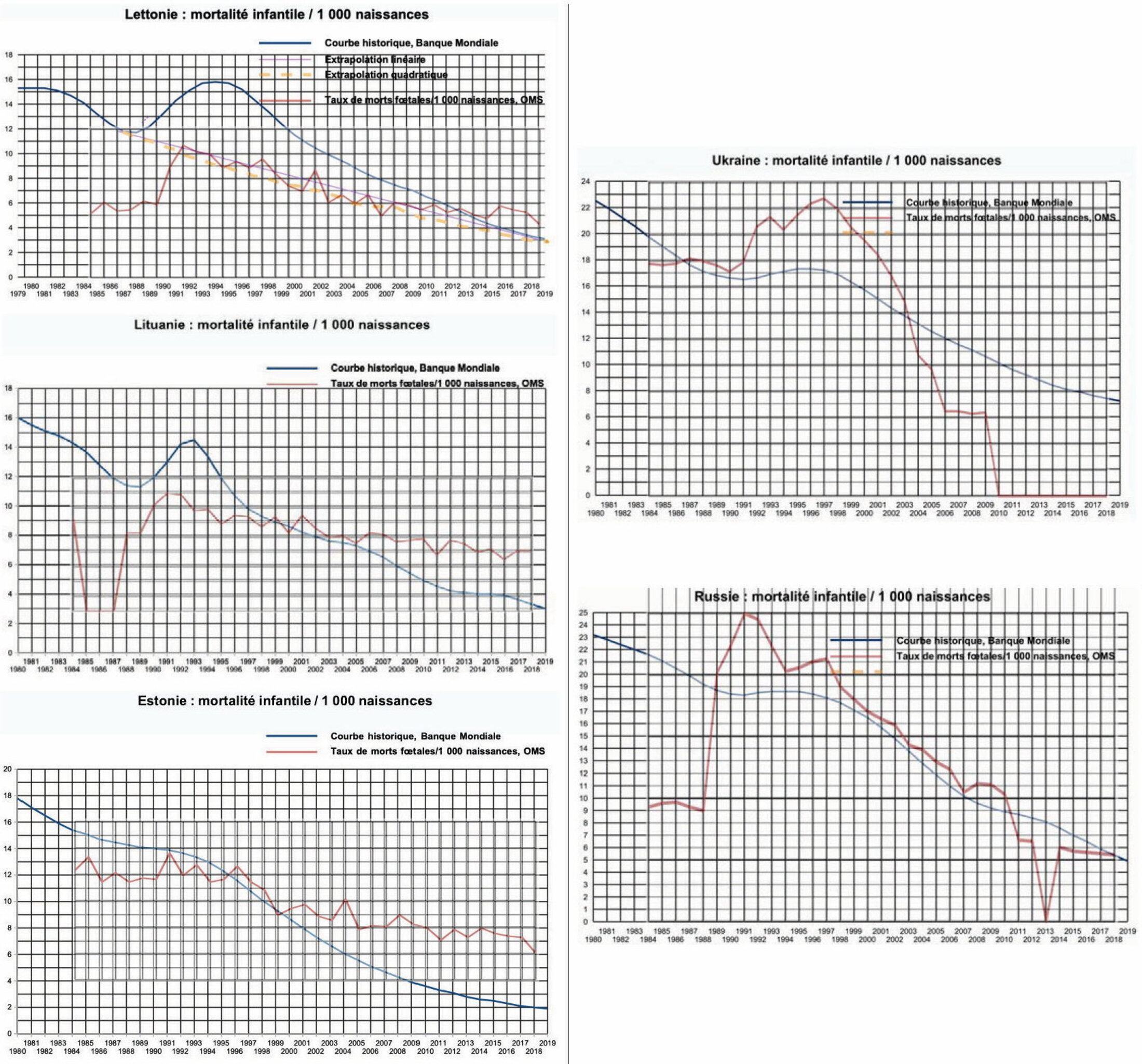
Comment 2
The three Baltic States did not suffer from fallout because it did not rain when the Chernobyl plumes passed over them. All three sent liquidators to Chernobyl.
However, Estonia's contribution was minimal due to the opposition of citizens to go to the site and the revolt of the 3,000-strong contingent when confronted with the conditions at the plant site.
In contrast, the Latvian contingent (over 6,000) and the Lithuanian contingent (over 7,000) were more seriously and long term exposed.
We do not know the detailed dosimetry of these groups of liquidators, and if we did, it would not allow any numerical inference since it is common knowledge that the registers were systematically falsified by default... it is easy to understand why.
The information that these three curves provide us with is essential: the anomalies have their sole origin in the return of the liquidators and the subsequent engravings during the couples' fertility period.
Comment 3
The quality of the health system in Russia and Ukraine was significantly lower than in Belarus and the Baltic States. It should be taken into account that the economic collapse after the break-up of the Union may have played a role in the dramatic increase in fetal mortality, especially in Russia. It should be noted that the deterioration of indicators started before the economic collapse. Chernobyl is therefore clearly involved.
A comparison with the developments in Belarus and the Baltic States will serve to weigh the role of Chernobyl in these disastrous performances.
A common feature of all these developments is that the fetal and infant mortality rates in all these countries are tending towards equal values, in the order of 4 to 6/1000, a development that reflects an equivalent level of quality of birth policy in all these countries, which are faced with the challenge of halting demographic decline by limiting losses during gestation and in the care of infants to a minimum.
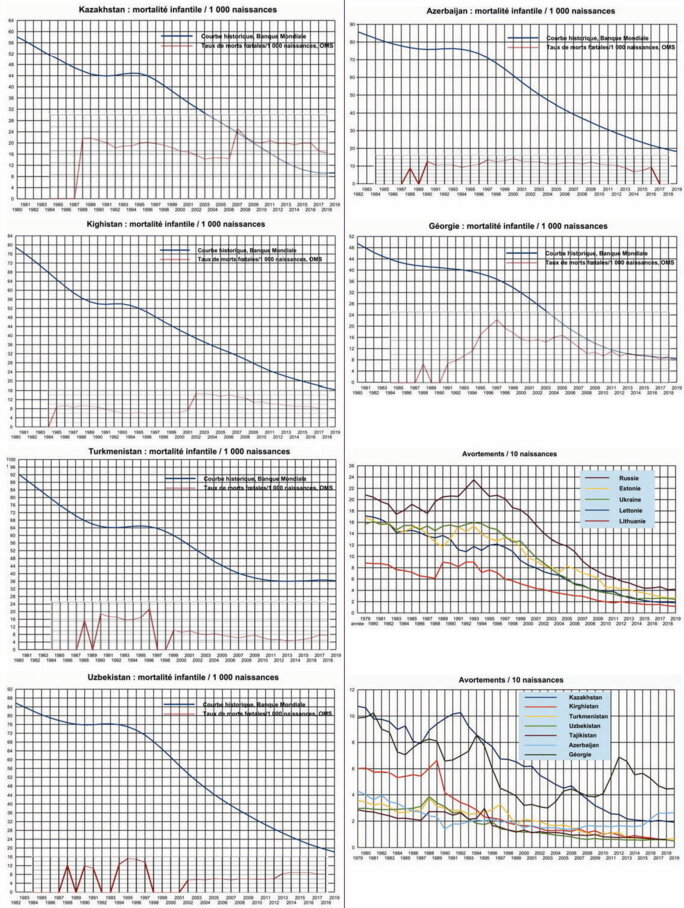
Agrandissement : Illustration 7
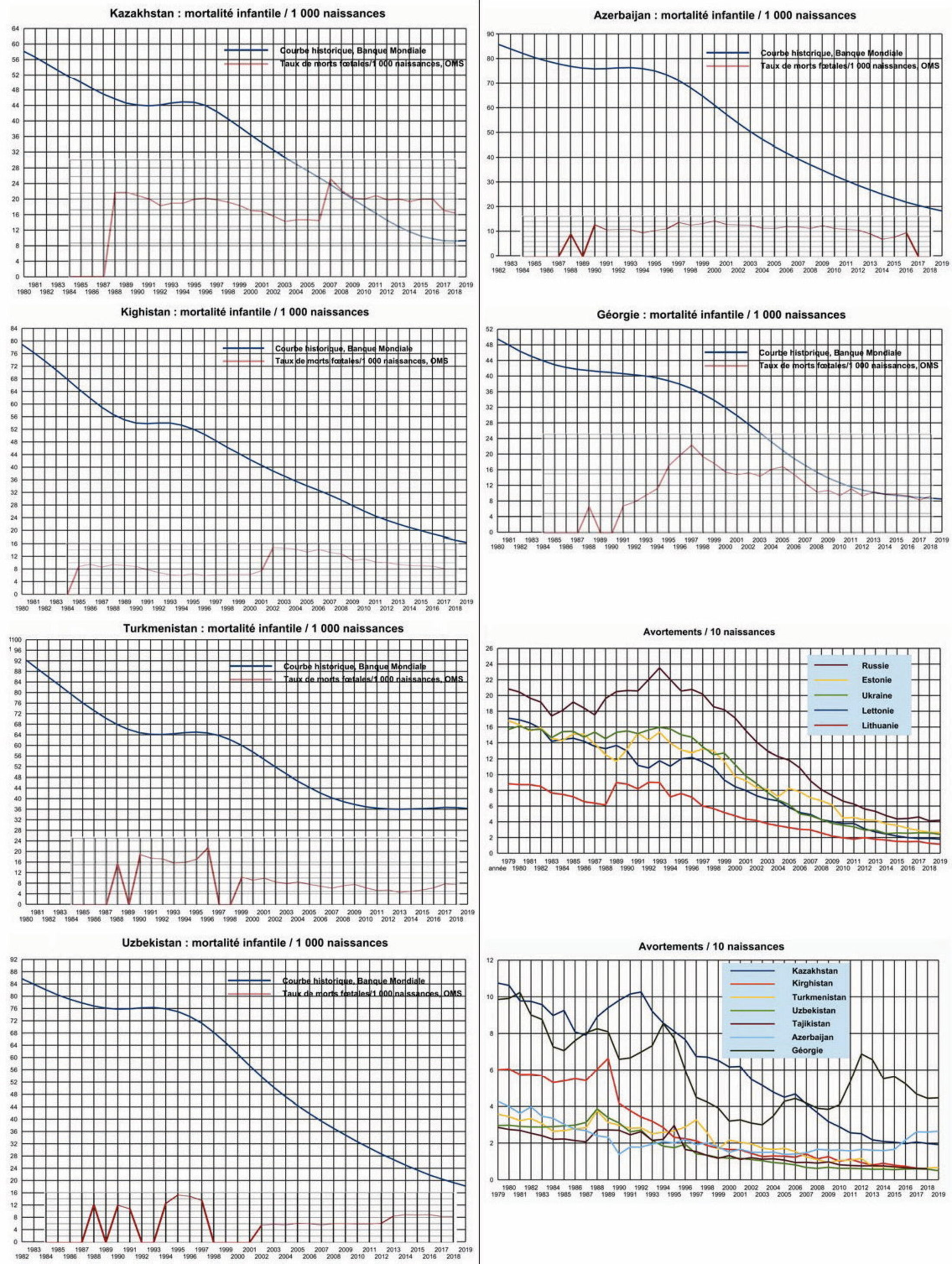
Comment 4
The Caucasian and Central Asian Republics are also affected by the effects of Chernobyl on the offspring of liquidators. There are also trend anomalies in therapeutic abortion rates, except in Azerbaijan (light blue curves). The post-2005 anomalies in the abortion rate in Georgia are certainly not due to Chernobyl; they may be a consequence of the conflicts with Russia that took place in this country, concluded by the 2008 annexations.
The influence of Muslim traditions is manifested in the very low rates of therapeutic abortions.
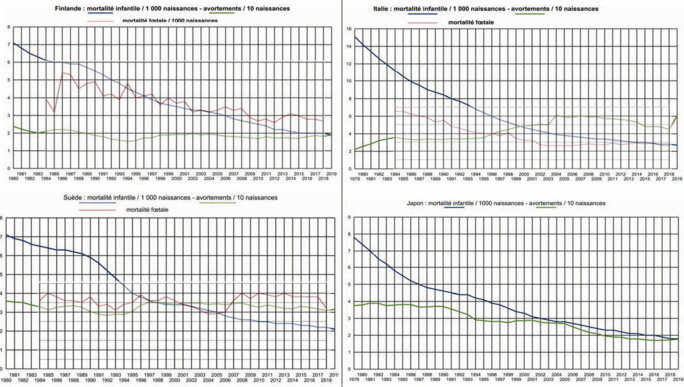
Agrandissement : Illustration 8
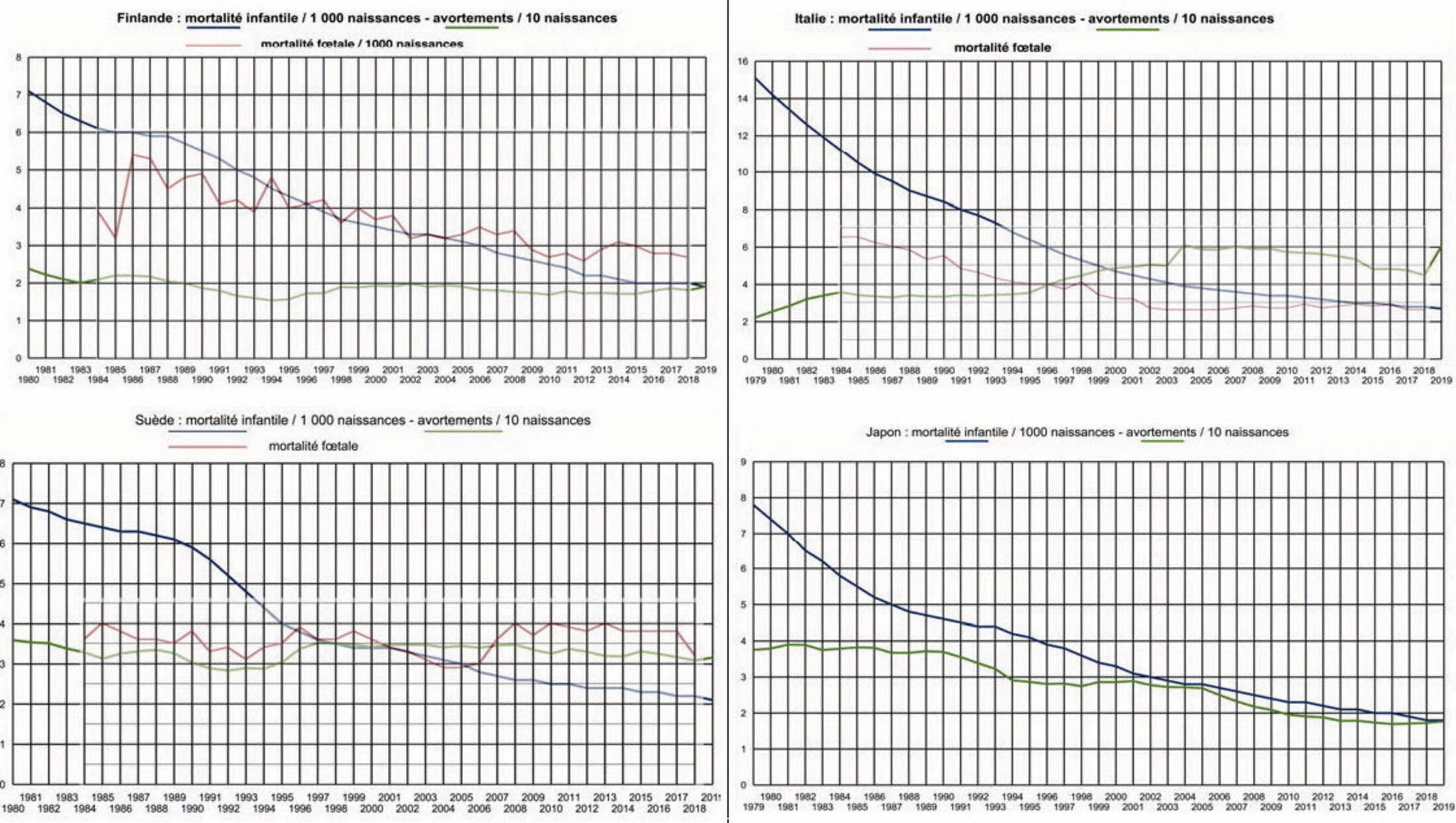
Comment 5
Both Finland and Sweden received significant radioactive fallout over parts of their territories. There are anomalies in the infant mortality rate curves. Therapeutic abortion rates are not affected.
In Finland, however, the number of fetal deaths seems to reflect a Chernobyl effect. As the data recorded by the WHO are incomplete, this can only be inferred with a moderate level of confidence.
Comment 6
There is no quantifiable Chernobyl effect on infant mortality curves, nor on therapeutic abortion curves in Italy and Japan. The decreasing trend of fetal deaths in Italy does not show any anomaly in the post-Chernobyl years (corresponding data are missing for Japan).
It is noted that there is no visible Fukushima effect on the infant mortality curve in Japan. This absence is certainly due to the excellent control of radioactivity in foodstuffs that the Archipelago benefited from after the radioactive fallout from the three explosions in March 2011.
Attempting to quantify abortions and fetal and infant mortality due to Chernobyl
The method we have used is the one described in the detailed treatment of the Belarusian case. The raw totals for the three types of damage are compiled in the table below, country by country.
The various cumulative figures for post-Chernobyl abnormalities in therapeutic abortions (the "angel" factory), fetal deaths (the undecided "angels"), and infant mortality (the "near-angels") have been collated, and these gross figures are related to the population of each country. Ratios are converted to absolute values by product with the number of annual births from international statistics.
Four groups of countries are distinguished:
- countries that sent liquidators and experienced radioactive fallout;
- countries that sent liquidators and did not suffer fallout, divided into two subgroups, those with a Russian culture and those with a Muslim culture;
- countries that did not send liquidators and suffered significant radioactive fallout;
- countries that did not send liquidators and did not suffer radioactive fallout.
The first group consists of Belarus, Ukraine and Russia.
The first sub-group of the second group includes the Baltic States, Georgia and Kazakhstan and the second sub-group includes the other Central Asian Republics plus Azerbaijan.
The third group consists of Finland and Sweden.
The fourth, the control group, is composed of Italy and Japan.
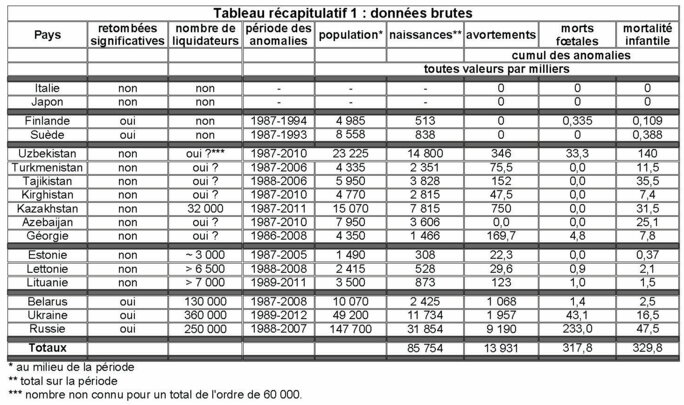
Agrandissement : Illustration 9
Discussion
1. The control group - Italy - Japan - is free of any anomalies. Poland could have been included notwithstanding a small area of fallout contamination in the north-east near the Russian enclave of Kaliningrad, an example of how, in the absence of wet fallout, there is no quantifiable impact on infant mortality.
2. The second group - Finland - Sweden - where the trend of therapeutic abortions does not show any anomaly, there are a few hundred (total slightly above 800) fetal deaths (Finland) and infant deaths (Finland, Sweden) spread over 6-7 years after the accident. The curves show this. However, it would be necessary to limit the statistics to the inhabitants of the sparsely populated regions that suffered the greatest fallout and to cross-reference the results with local dietary habits. This is feasible but beyond the scope of this very preliminary study.
3. From the third group we extract a group of Muslim countries where the curves of therapeutic abortions show no or few abnormalities after the accident, namely (abortion abnormality rate in %) - Azerbaijan (0.0); Kyrgyzstan (1.6); Tajikistan (3.9); Turmenistan (3.1) and Uzbekistan (2.3).
The number of liquidators mobilised in the Central Asian republics is not well known. It is known that a significant proportion was made up of military personnel whose various laws from June 1986 onwards prohibited any disclosure of information - numbers, doses received, mortality. Concerning mortality, we have a first-hand account from Professor Michel Fernex:
"Thus, in Kazakhstan more than 5000 kilometres from the destroyed reactor, in a barracks in the Semipalatinsk steppe, large panels bore the names of fallen soldiers, either in the Great Liberation War, in the Afghan War, and for the last panel, the officer who was leading us asked:
– "Do you know what it represents?
– No, I do not.
– It's our soldiers who were victims of Chernobyl."
Assuming the published figure of 90,000, including the 32,000 from Kazakhstan, 60,000 are retained for all five republics. The aggregate data for the period 1987-2010 are then
- births: 27,000,000 ;
- abortions: 621,000 (2.3%);
- anomalies fetal deaths: 33,000 (1.2‰) ;
- anomalous infant mortality 219,000 (8.1‰) to be put into perspective with the 75‰ figure for average infant mortality in those years.
These figures show that the Chernobyl effect is diluted in another effect, that of the disruption of health services in the decade or so following the break-up of the USSR. For the orders of magnitude of all these anomalies are incompatible with the number of 60,000 liquidators. The distribution of contaminated food from the highly contaminated regions of the Russian Federation, Ukraine and Belarus may also have played an important role as it is known that the pursuit of the Plan's objectives remained a priority, including in agricultural production. So, in the absence of information on the subject and thinking themselves safe because of their distance from the Chernobyl plant, most pregnancies were carried to term without systematic and exhaustive prenatal examinations.
Assuming a kind of "compensation", namely that the reduction in prenatal examinations caused by the economic difficulties affecting these years resulted in a small increase in therapeutic abortions and thus in an increase in fetal and infant deaths, it is proposed that the total - 873,000 (3.2% of births) - of the above figures should be taken as measuring the Chernobyl effect on the birth rate in these five Central Asian Republics. This is a maximum.
Assuming that the economic crisis had much more devastating effects, and that only one therapeutic abortion is retained on average in the offspring of each liquidator, and the rest in proportion, then the total effect of Chernobyl on the birth rate would be more like 100,000.
Finally, we know that the USSR's troop engagement doctrine favours sending young, inexperienced conscripts to the front line. Testimonies from the time show that this was the case during the Chernobyl war. The young soldiers who survived long enough to start a family would not have had their first children until several years after Chernobyl, after they had married. This is true for all contingents and would explain why the anomalies only peak around 1995, whereas in Finland and Sweden it is earlier, in 1989-1990.
4. Kazakhstan and Georgia are characterised by a fairly marked anomaly in the number of therapeutic abortions, respectively 9.6 and 11.5% of total births. This is necessarily a general trend in the whole population of which only about 2‰ are Chernobyl liquidators. However, the low total of abnormal fetal and infant deaths - 44,100 (4.7‰ of births) is not inconsistent in magnitude and causality with the number of liquidators, 32,000 for Kazakhstan alone, the figure for Georgia not being known to us.
5. The three Baltic States - Estonia, Latvia and Lithuania - sent a rather small proportion, 2.1‰, of their population to Chernobyl, 16,000 liquidators. These countries had a long tradition of a very high level of medical care and prenatal monitoring. It is assumed that the quality of these health services has not been significantly altered by the economic difficulties of the 1990s. The abortion anomalies are respectively 7.2 - 5.6 and 14% of births to be distributed over the 20 or so years of the period concerned. The total number of anomalous fetal and infant deaths is low, 5,870, which, if related to the number of liquidators, means one death from these causes for every three liquidators. On the other hand, the size of the increase in abortions suggests a psychological reaction: not to take the risk of having a malformed child, given that not all congenital malformations are visible on ultrasound. Should the "angels" thus "produced" be excluded from the count of accident victims? No, if the accident had not occurred, neither would these abortions, because no woman terminates her pregnancy without a compelling reason if she wanted the child to be born.
The interest of this group is to quantify with a good degree of certainty the order of magnitude of fetal losses and infant deaths in the descendants of the liquidators. The total of the three causes, abortions, fetal deaths and infant mortality in the three Baltic States thus amounts to 180,000 in the period 1987-2011.
6. The last group includes the most affected countries and these are also the ones that made up the bulk of the liquidator contingents, 740,000 in total. The cumulative anomaly of fetal and infant deaths is 344,000, a proportion consistent in magnitude with that of the Baltic States, bearing in mind that the doses received by evacuees and the effect of the fallout are not to be neglected.
If we retain the proportion for the Baltic States, then 246,000 of the 344,000 fetal losses and child deaths occurred in the descendants of the liquidators. This leaves just under 100,000 caused by fallout and doses received by evacuees. As for the fallout, applying the ratio of anomalies to births in Finland and Sweden by a rule of 3, without adjustment, we would have 31,000 losses to attribute to it. This leaves 70,000 to be divided between the doses received by the evacuees and the greater effect of more intense fallout. There is a certain consistency in all these assessments.
On the other hand, the "catastrophic" number of abnormalities on the abortion curves is certainly not entirely due to the detection of malformations on ultrasound. The considerable difference between the proportion of abortions in the Stolin raion compared to those in the Brest oblast and, more generally, in Belarus as a whole, argues for a disproportionate political decision. Indeed, Dr Raisa Misura and the services under her command have had a constant preoccupation with supporting the birth rate, and, as she has made clear, justifying every abortion by a malformation detected on ultrasound. The bulletin of the UN office in Belarus praised the results achieved. However, there are no statistics on abortions in this raion prior to 1986. To assess the number of these motivated abortions would require compiling the records of its central hospital...
It appears that, as a country with a highly contaminated surface area and population, Belarus has the highest cumulative abortion anomalies: roughly speaking, 1 abortion per 2.5 births between 1986 and 2008. The figures for Ukraine and Russia are lower in proportion, but considerably higher in absolute values, due to much larger populations: 1 abortion for every 3.5 and 6 births respectively in Ukraine and Russia, for a total of 11 million abortions for 42.5 million births.
Without the accident, these abortions would not have been induced. Their cohort constitutes the bulk of the celestial legions of Chernobyl "angels".
An impossible balance sheet
To conclude would be the nonsense of nonsense. Based on an inadequate vision of the aftermath of a major radiological crisis, with the small cohort of Hiroshima and Nagasaki survivors as the only reference, and without taking into account in their analysis the very small amount of lasting fallout in the "black rain" zones, but also in order to absolve the accident of such consequences, the official reports of the UNSCEAR, the ICRP, the WHO, and their repetition by all the institutions such as the IAEA, the OECD, etc. only mention increases in the number of congenital malformations, as a result of better detection. In short, the international experts tell us that thanks to Chernobyl the medical institutions of the most affected countries have made great progress. The words fetal (for fetal death) and abortion are absent from the WHO summary report published in April 2006 under the title Fact Sheet WHO 303, Health Effects of the Chernobyl Accident, an Overview, of which the following extract, placed just before the last paragraph, exhausts the question of malformations:
"Reproductive and hereditary effects and children's health
Given the low radiation doses received by most people exposed to the Chernobyl accident, no effects on fertility, numbers of stillbirths, adverse pregnancy outcomes or delivery complications have been demonstrated nor are there expected to be any. A modest but steady increase in reported congenital malformations in both contaminated and uncontaminated1 areas of Belarus appears related to improved reporting and not to radiation exposure.
WHO's role
The Expert Group report is a milestone in WHO's efforts to assess and mitigate the health impact of the Chernobyl accident. WHO will actively promote the research and practical recommendations given in this report. In addition WHO will ensure that the people most affected by the Chernobyl accident will be provided with scientifically factual information that will allow them to make better informed decisions about their health and future."
The UN thus concluded: this is indeed the nonsense of nonsense.
Notes
1 - Member of the Interdepartmental Group on Radioactive Waste (1974-1975)
- Co-expert of the Lower Saxony Government for the Gorleben atomic complex project (1978-1979)
- Member of the Steering Committee of the parliamentary mission on the health effects of radioactive waste chaired by Michèle Rivasi (2000-2001)
- President of the international association Children of Chernobyl Belarus(2010 - )
- co-author, with Hélène Crié, of the techno-thriller Tchernobyl sur Seine, Editions Calmann-Lévy (1987)
- author of La Comédie Atomique, Editions La Découverte, 2016
- author of the film Tchernobyl, le monde d'après, directed by Marc Petitjean, 2018
2 "The following is a description of the child health groups in Belarus:
Health groups depend on:
1. Developmental characteristics (genealogical, biological and social history - data obtained during patient examination).
2. The level of physical and neuro-psychic development.
3. The degree of resistance of the organism to diseases.
4. The level of functional status of the main body systems.
5. The presence or absence of chronic diseases or malformations.
By considering each element, the paediatrician determines the child's health group and enters it in the medical record.
Health group" is a conditional term. In medical practice, it is used to establish action plans for the rehabilitation and education of children. For children of primary and pre-school age, there are five such groups.
The first group includes children who do not show deviations in their health status. The physical development of these children is harmonious and corresponds to their age, they rarely fall ill, illnesses are easy.
The second group consists of children with some kind of functional disorder, most often associated with uneven growth and development. For example, functional systolic heart murmurs, mild postural disorder, mild deficiency or excess body weight. These children fall ill up to four times a year.
The third health group includes children with chronic diseases in the compensatory stage (the body adapts to changes due to the disease).
The fourth group - children with chronic diseases in the sub-compensation stage (after an exacerbation of the underlying disease, general condition and well-being are disturbed for a long period of time).
The fifth health group includes children with chronic diseases in the decompensation stage. This group also includes children with disabilities. These children do not usually attend general pre-schools."
Dr Alexey Nesterenko, Director of the BELRAD Institute of Radiological Protection.
3 The team composed of Dr. A. V. Nesterenko, director of the BELRAD Institute, R. and M. Hugot and Y. Lenoir from the NGO Children of Chernobyl Belarus.
4 The population of the raion is around 90,000, of which approximately 15,000 live in the capital.
5 Raisa Misura retired in 2019 but continues to practice as a paediatrician, her primary vocation.
6 By "near-angels" I mean children who died in their first year, those who fall under the heading of "infant mortality".
7 Indicative data. Ukraine: 360,000; Russia: 250,000; Belarus: 130,000; Kazakhstan: 32,000; Latvia: >6,500; Lithuania: >7,000; Armenia: 3,000. Several tens of thousands are missing from this count. Moreover, the number of soldiers, most of them very young or reservists (the best troops were deployed in Afghanistan at the time), sent to the site between May and July 1986, who were the most exposed, is not clear: the figure of 350,000 has been put forward; the 2008 UNSCEAR Annex D report gives a figure of 240,000. The doses received by the soldiers are covered by secrecy.
8 Zr95 (period: 65 days), Ru106 (1 year), Ce144 (265 days), Pm147 (2.6 years) and activation products such as Mn54 (300 days), Fe55 (2.9 years), Co60 (5.2 years). Even Sr90 (28 years) remains little considered because it is impossible to measure in the body, except after autopsy and specific sampling.
9 <http://www.johnstonsarchive.net/policy/abortion/index.html#BS>